Share:
When I lead in-person education sessions on wheelchair cushions, one of the questions that I am frequently asked is, "How do you get staff to put the cushions on the correct way?" When the cushion is removed from the wheelchair to clean the cover and/or the cushion base, mistakes sometimes occur when replacing the cushion base in the cover and/or when replacing the cushion on the wheelchair. I have heard of cushions being put on upside down and front-to-back on wheelchairs, despite the training provided by therapists on correct cover and cushion placement. Since this question continues to come up, I thought I would address this issue in this month's Clinical Corner article, using concepts from adult learning theory and knowledge translation. (If you are wondering why I chose to use these concepts, see my bio here).
Let's first look at knowledge translation, or KT. Typically, KT is applied to the creation, dissemination and use of knowledge based on evidence, such as systematic reviews. In fact, the definition of KT is "a dynamic and iterative process that includes synthesis, dissemination, exchange and ethically-sound application of knowledge to improve the health of Canadians, provide more effective health services and products and strengthen the health care system".
The model below, retrieved from the Canadian Institutes of Health Research (CIHR) website, helps to illustrate the knowledge to action process:
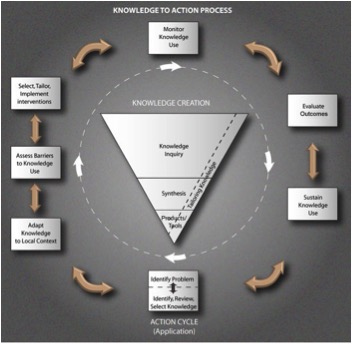
(Canadian Institutes of Health Research, 2015)
For the purpose of looking at staff training and wheelchair cushion placement, we will not place a lot of focus on the knowledge creation cycle, illustrated by the funnel, or inverted triangle, in the Knowledge to Action Process model. While the model conceptualizes research-based knowledge, other forms of knowing, such as experiential knowledge, also apply to this model.2 In our example, we are using experiential and clinical knowledge of wheelchair cushions. Let's now look at the action cycle, or the application of knowledge.
As you can see in the above model, the action cycle is comprised of 7 action phases, which can occur sequentially or concurrently.3 These action phases include: identifying the problem and selecting the appropriate knowledge to apply; adapting knowledge to the local context or environment; assessing the determinants of knowledge use – both barriers and supports; selecting and tailoring interventions to transfer knowledge; monitoring knowledge use; evaluating outcomes; and sustaining knowledge use. Let's look at each of these phases and see how the knowledge of correct wheelchair cushion placement can be transferred and sustained when working with caregiving staff members.
Identifying the Problem and Selecting Knowledge
This is an easy one for us to address with our example. The problem is that cushions and their covers are not correctly placed on wheelchairs on a consistent basis after the cushion and/or cover has been cleaned. The knowledge that we will be applying is our clinical knowledge of correct application of a cushion cover on a cushion base (remembering that a cushion cover is integral to the design of a cushion – we do not want to see pillow cases acting as cushion covers!) and of correct cushion placement on a wheelchair (e.g., orientation of a pelvic loading area well and/or contours with respect to a wheelchair seat pan).
Adapt Knowledge to Local Context
Before we undertake big actions to change the practice of all caregivers, we want to find out the extent of the problem. Where is it that the issues are occurring? Is it in mismatched cushion covers and bases? Is it lack of understanding cushion contours and their purposes? Or is it that the task of putting a cushion onto a wheelchair is too routine? It has been found that "what most individuals do most frequently is what they think about the least."4 (p. 104). Is the problem isolated to particular individuals? Once the context is known, clinical knowledge related to wheelchair cushions can be targeted to best suit the circumstances at particular facilities.
Assess Barriers and Facilitators to Knowledge Use
Next, we assess the determinants of knowledge use – what helps or hinders staff from placing cushions correctly on a wheelchair? Generally speaking, barriers cited for knowledge use in healthcare include knowledge (e.g., lack of awareness, forgetting); attitudes (e.g., lack of motivation to change one's habits); and behavior (e.g., external barriers, such as time pressure and lack of resources).5 Think about this in the local context. Caregivers are caring people and want to do what is correct for the client so likely attitude is not the issue. Knowledge and external factors, such as perceived lack of time or lack of clean, appropriate cushion covers, may be the issue.
Select, Tailor and Implement Interventions
There are many different knowledge translation interventions. Some interventions are formal education sessions, such as large group, small group and 1:1 sessions; audit and feedback interventions; and organizational interventions. Using multiple strategies addresses a wide range of determinants of knowledge use.6
When implementing education sessions, whether for a large or small group, it is important to consider adult learning theory. People have different learning styles. While a "lecture" and demonstration may work for one individual to understand the knowledge and change practice based on the visual and auditory message, another person may require experiential learning through hands-on and feeling what it is like to sit on a cushion that is placed properly versus improperly.
Some people may require a visual cue as a follow-up reminder of the education. For example, many wheelchair cushions have labels on the base of the cushion and on the outer cover to label the front and back of each, but even this is sometimes not enough. Perhaps the words need to be written in bigger font with a permanent pen on both the cushion base and the cushion cover for some individuals.
If the barrier is lack of clean, appropriate cushion covers (specific to each cushion base), the strategy required may be on more of an organizational level to ensure that there are the resources in place to have secondary cushion covers (specific to each cushion base) available for when an equipment pool cushion cover is being laundered. For individuals who are prescribed their own cushions and wheelchairs and who are incontinent, a second cushion cover should be prescribed so that it can be placed on the cushion while the other is being laundered, again ensuring that the cushion base and cover are properly labelled with front and back.
Monitor Knowledge Use and Evaluate Outcomes
In our example, we must continue to monitor the effects of our staff training. Since our example is straightforward, an easy way to monitor knowledge use and to evaluate outcomes is to determine the frequency with which wheelchair cushions continue to be placed incorrectly on wheelchairs.
Sustain Knowledge Use
Sustaining knowledge use refers to the continued implementation of the knowledge that is transferred and planning for ways to ensure the sustainability.7 We cannot assume that we can provide knowledge translation interventions, such as education sessions, only once and that it will be sufficient to change behaviours. In our example, we must plan to continually ensure that new staff members have the knowledge and skills to place the wheelchair cushions properly on the wheelchairs.
Summary
This month, we looked at the issue that sometimes wheelchair cushions are not placed properly on a wheelchair after the cushion or cover has been cleaned, despite staff training. We used the Knowledge to Action Process model to look at the different steps we should consider in knowledge translation to effect a sustainable change in behaviour and to realize that one intervention alone will not be sufficient to prevent misplaced wheelchair cushions. We also looked at the importance of understanding individuals' different learning styles when we develop educational strategies for caregiving staff and to understand that in order to find unique solutions for the facilities in which we work, we need to understand the unique circumstances in each facility.
References
- Canadian Insitutes of Health Research. (2015, September 29). About us - Knowledge translation. Retrieved from http://www.cihr-irsc.gc.ca/e/29418.html.
- Sudsaward, P. (2013, November 20). Knowledge Translation: Introduction to Models, Strategies, and Measures. Retrieved from http://ktdrr.org/ktlibrary/articles_pubs/ktmodels/.
- Strauss, S., Tetroe, J., & Graham, I.D. (2013). Introduction. Knowledge translation: What it is and what it isn't. In. S.E.Straus, J. Tetroe, & I.D. Graham (Eds.), Knowledge translation in health care. Moving evidence to practice (pp. 3-13.). Oxford: Wiley-Blackwell.
- Kitson, A.L. & Straus, S.E. (2013). Identifying knowledge to action gaps. In. S.E. Straus, J. Tetroe, & I.D. Graham (Eds.), Knowledge translation in health care. Moving evidence to practice (pp. 97-109). Oxford: Wiley-Blackwell.
- Legare, F. & Zhang, P. (2013). Barriers and facilitators. In. S.E. Straus, J. Tetroe, & I.D. Graham (Eds.), Knowledge translation in health care. Moving evidence to practice (pp. 121-136). Oxford: Wiley-Blackwell.
- Wensing, M., Bosch, M., & Grol, R. (2013). Developing and selecting knowlede translation interventions. S.E. Straus, J. Tetroe, & I.D. Graham (Eds.), Knowledge translation in health care. Moving evidence to practice (pp. 150-162). Oxford: Wiley-Blackwell.
- Davies, B., & Edwards, N. (2013). Sustaining knowledge use. In. S.E. Straus, J. Tetroe, & I.D. Grahams (Eds.), Knowledge translation in health care. Moving evidence to practice (pp. 237-248). Oxford: Wiley-Blackwell.